Memorial Hermann's Population Health Service Organization's Health Management department is designed to support patients, families, physicians and health care professionals by improving the overall health of our assigned ACO lives. Our team performs a comprehensive assessment and provides individualized care plans to meet the specific needs of the individual by collaborating with physicians, clinical staff, patients, family members and caregivers.
The Health Management Department works to achieve this goal by supporting and educating ACO-assigned patients on their acute and chronic health care conditions. We assist patients by promoting health wellness and health prevention to help decrease the chances of visiting the hospital or emergency room unnecessarily. Our team will assess all medical and psychosocial needs and work to help overcome any barrier that would prevent a patient from reaching their optimal health. With this knowledge, patients feel empowered to manage their own care and communicate with their providers about their individual needs.
Our multidisciplinary team includes experienced Registered Nurses, Licensed Vocational Nurses, Social Workers, Pharmacists, Community Health Workers, Health Coaches and Non-Clinical Support Staff who are dedicated to meeting the needs of our patients and their families through ongoing support and care coordination.
A Multidisciplinary Care Coordination Team
Experienced Registered Nurses, Licensed Vocational Nurses, Social Workers, Pharmacists, Community Health Workers, Health Coaches and Non-Clinical Support Staff are committed to providing comprehensive education and support to ACO-assigned patients and their families. Our goal is to optimize your health and wellbeing while in your community setting.
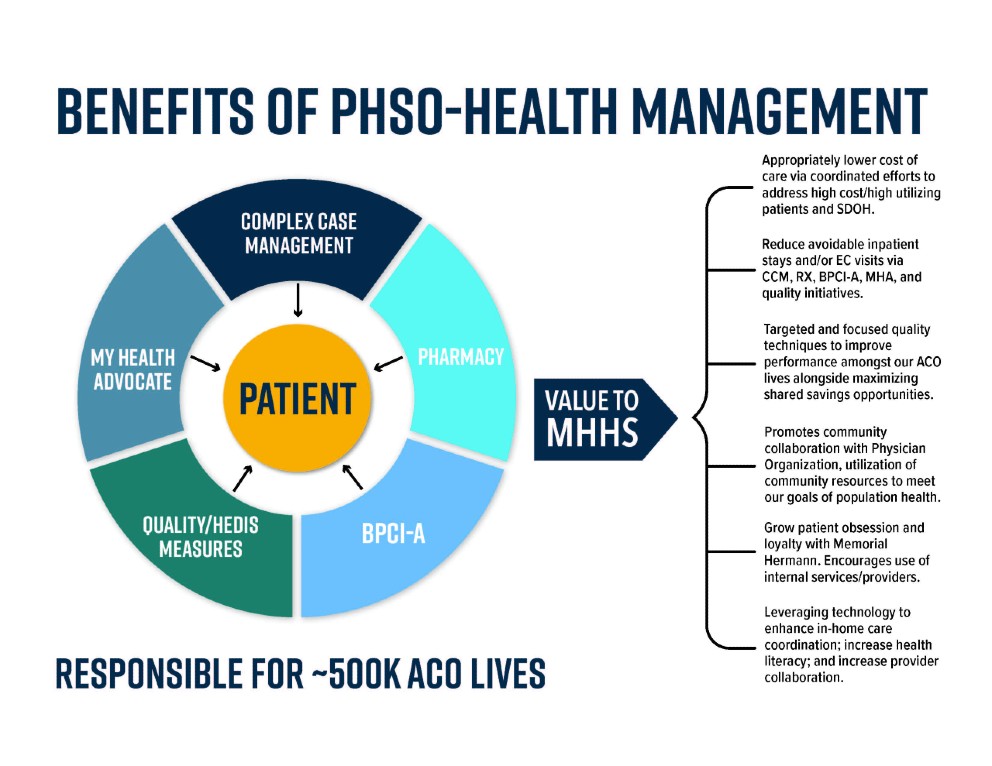
Health Management Programs
Complex Case Management
Complex Case Management is a collaborative process that assesses, plans, implements, coordinates, monitors and evaluates the options and services required to meet the patient’s physical, emotional and mental wellbeing.
- Assessment of medical, functional and psychosocial needs
- Development of an individualized plan of care to improve overall health
- Provides education and support for all disease processes
- Works with your primary care physician and specialist to coordinate care
- Provides Transitions of Care support post-hospitalization to include:
- Review and understanding of discharge paperwork
- Assistance with post-discharge follow-up appointments
- Medication reconciliation
- Assessment of barriers and/or challenges to actively participating in care
- Referrals to other team members as needed for support (Pharmacists, Social Workers, Health Coaches)
- Enhance coordination of care in the medical and social environments
- Ongoing telephonic support
- Provides social work support to connect you with community, home, behavioral or other identified resources
- Addressing completion of preventive and wellness screenings
- Assistance with appointment scheduling
Bundled Payment for Care Improvement Advanced (BPCIA)
BPCIA is a program within the Health Management Department dedicated to providing transitional coordination of care services. We are committed to managing and supporting the BPCIA population through comprehensive case management.
- A Centers for Medicare and Medicaid (CMS) value-based program that provides a single, comprehensive payment covering all services provided during a patient’s 90-day episode of care.
- Onsite and telephonic Transitional Care Managers provide transitional case management and care coordination for eligible bundle patients with moderate to complex care needs.
- Comprehensive case management is provided throughout the 90-day care episode, including Skilled Nursing Facility, Inpatient Rehabilitation and Long-Term Acute Care transition of care, with the goal of reducing readmissions, decreasing emergency room utilization and improving patient outcomes.
- Care Management includes comprehensive onsite patient assessment, identification of gaps and Social Determinant of Health barriers to care, patient centered goals and a multidisciplinary team approach.
- Multidisciplinary team members include Transitional Care Managers, Post-Acute Care Coordinators, Social Workers, Pharmacists, Community Health Workers and Health Coaches.
- Program eligibility is determined by CMS criteria of Medicare Part A and Part B, as well as an identified eligible Bundle diagnosis. General referrals to the program are not accepted at this time.
Remote Patient Monitoring
My Health Advocate (MHA) is a Memorial Hermann remote patient monitoring program that helps patients living with heart failure, lung disease, diabetes and/or COVID-19 to better manage their conditions at home by:
- Using technology to monitor in real time patient’s health and wellbeing
- Dedicated team to monitor, support and educate patient daily
- Providing important health information to your physician
- Goal is to decrease the chances of having to visit the hospital or emergency room
Pharmacy
Clinical Pharmacy Services (CP) are patient-oriented activities developed to promote the appropriate use of medication, reduce financial burden, overcome barriers, and optimize therapeutic outcomes while ensuring safe and effective medication use for each patient. The CP offers:
- Medication Therapy Management (MTM): Designed to offer comprehensive medication reconciliations for our ACO and BPCIA populations.
- Utilization Management: Provides more cost-effective alternatives and drug recommendations to your provider.
- ACO Quality Measure: Program focuses on medication-driven metrics to encourage patient compliance and support quality gap closure.
Health Management Interventions
- Care Coordination support for ACO-assigned lives either telephonically or face to face
- Tools and education to successfully monitor and manage your health
- Regular contact from a Health Management staff person depending on need
- Medication education and review
- Assess for needs that would benefit from resources and referrals
- Optimize patient’s health and wellbeing via coordinated care
Contact Us
If you have questions regarding the programs offered by Health Management, please call us at (713) 338-5353 Monday-Friday between 8 a.m. and 5 p.m. Please allow 2 business days for a return call from a member of the Health Management staff for messages left on the secured voicemail system. You can also reach us via email at Healthmanagement-PHSO@memorialhermann.org.